
Managing Concussions in Ultimate
You’re on the sidelines at practice when a huck goes up and two of your teammates collide laying out for the disc. One gets up quickly, but the other, who looked like she hit her head pretty hard, is taking longer to get up. You rush over to help, but when you get there you realize you’re not sure what to do next…
I would guess that many of us have been in a similar situation. Instinctively, we suspect a head injury such as a concussion, but we’re not sure what to do about it. We might ask if they remember what day it is or to look at how they are walking. What do we hope to gain from these things? How do you know if they should go the emergency room? Is it really a concussion? Can they get back out on the field?
Here’s a quick look at what concussion management in ultimate should look like:
- Initially, 24-48 hours of rest. See a medical professional during that time.
- Assume a suspected concussion is a concussion. No athlete should resume playing ultimate the same day they may have gotten a concussion.
- Begin a gradual return to play program based on symptoms.
- Search for providers trained in concussions, neurology, or vestibular disorders
If you want a bit more detail about these points, read on!
We’ll start with a definition. According to the 5th International Conference on Concussion in Sport, “sport related concussion is a traumatic brain injury induced by biomechanical forces.”1 In ultimate, athletes may get a concussion through collision, whiplash from laying out, or even getting hit in the head with a disc! If we look at the literature regarding injury rates in ultimate players, concussions are fairly common.2-4 A 2018 study surveyed ultimate players and found that about 25% of respondents had previously suffered a concussion!5
There a variety of things about our sport that make proper medical management of concussion difficult. The absence of dedicated medical staff, the lack of specific education about concussions, and the fact that not all teams have coaches are a few reasons concussions are a such problem in ultimate. Concussions are often under reported in other sports6-8 and a similar trend is probably present in ours. In addition, the same 2018 study by Lazar, Lichtenstein, and Tybor found that around 40% of ultimate players surveyed returned to play on the same day as their head injury.5 If ultimate players received proper concussion management, this number would be 0%.
"Around 40% of ultimate players return to play on the same day as their head injury. If ultimate players received proper concussion management, this number would be 0%"
Concussions increase the risk of other injuries
When mismanaged, concussion has the potential to cause serious health problems. After a concussion, athletes are at a greater risk of musculoskeletal injury, including ligament sprains, muscles tears, and other more typical sport injuries.9, 10 One literature review found that after suffering a concussion, athletes were more than 2 times as likely to suffer a musculoskeletal injury such as an ACL ruptures!9 On the other hand, athletes who receive adequate treatment after a concussion return to sport faster with fewer side effects.11, 12
Though instinctively we cringe at injuries such as an ACL tear, there are some even scarier possibilities when it comes to concussion. Second impact syndrome is a poorly understood, but potentially fatal injury that can occur if an athlete suffers another hit before the previous concussion heals.13, 14
Post-concussion syndrome occurs when a concussion continues to cause side-effects such as headache, fatigue, reduced cognition, dizziness, and many other symptoms for months or even years following concussion. The likelihood of post-concussive syndrome may increase with poorly managed concussion recovery.15, 16
Sometimes it can be difficult to understand how significantly these potential side effects could affect your life, but small things like fatigue and reduced cognition can significantly impact success in school or at work for years to come.
So you think a teammate just may have just suffered a concussion, what do you do?
If there is an athletic trainer or other qualified healthcare provider present, they should be notified and allowed to assess the athlete as soon as possible.
If not, you should assess the athlete for any signs or symptoms of injury. By talking to the athlete, you can get an idea if something more serious is going on.
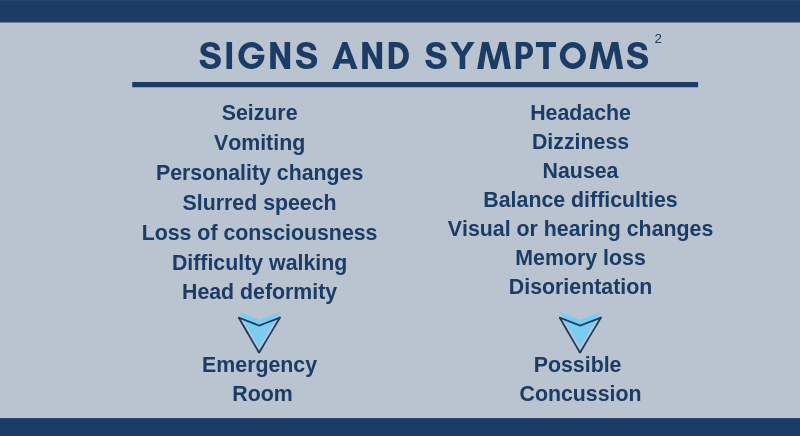
If any of the symptoms in the first column above are present, the athlete should be taken to nearest emergency department.1
If the athlete doesn’t display any of those symptoms, they probably do not need an emergency room visit, but they may still have a concussion! Look out for the common signs and symptoms of concussion listed in the second column.17
If you suspect a concussion, the best thing you can do is to make sure the athlete does not return to play for the rest of the day. Athletes showing symptoms of concussion should not return to play on the same day as the injury. Even without any of these symptoms, a concussion is still possible. Unless cleared by a medical professional, any athlete suspected of having a concussion should be removed from play for the rest of the day.1, 18
Even after reminding them of the increased risk for serious musculoskeletal or brain injury, athletes without symptoms will often insist they are ready to play the same day. In these situations, it is important to consider two things.
- Symptoms of concussion may not present immediately, instead developing over a few hours following injury.1, 18
- There are no definitive concussion tests.1, 18
This makes it is extraordinarily difficult to be certain an athlete has not sustained a concussion without the help of a medical professional.
It’s the day after a concussion. What are the next steps?
The first step is finding a healthcare provider who specializes in concussions. Physicians, physical therapists, chiropractors, and athletic trainers are examples of medical professionals who can treat concussions. There are different concussion subtypes that may affect vision, balance, cognition, or other areas that can be treated with specific techniques and exercises. It is a serious injury and should be rehabilitated with guidance from a professional like any other serious injury.

Up until recently, strict rest was the treatment of choice for concussions. In the last few years, a growing body of evidence suggests that resting for more than a few days can prolong recovery following concussion! Current best practice is an immediate rest period of 24-48 hours, followed by a gradual return to play program, consisting of progressive, symptom-free exercise.19-21 The following table is taken directly from the 5th International Conference on Concussion in Sport.1
Return-to-Sport Progression
|
Stage |
Aim |
Activity |
Goal of each step |
|
1 |
Symptom-limited activity |
Daily activities that do not provoke symptoms |
Gradual reintroduction of work/school activities |
|
2 |
Light aerobic exercise |
Walking or stationary cycling at slow to medium pace. No resistance training |
Increase heart rate |
|
3 |
Sport-specific exercise |
Running or skating drills. No head impact activities |
Add movement |
|
4 |
Non-contact training drills |
Harder training drills, e.g. passing drills. May start progressive resistance training |
Exercise, coordination and increased thinking |
|
5 |
Full contact practice |
Following medical clearance, participate in normal training activities |
Restore confidence and assess functional skills by coaching staff |
|
6 |
Return to sport |
Normal game play |
There should be at least 24 hours (or longer) for each step of the progression. If any symptoms worsen during exercise, the athlete should go back to the previous step. Resistance training should be added only in the later stages (stage 3 or 4 at the earliest).1
What can you do now?
If you are a part of a team, educate your teammates about concussion recognition, treatment, and management. Find a local healthcare provider to come give a presentation to your team about concussion management. A team full of people educated about the severity and management of concussions will be more likely to support teammates in choosing good concussion management.
Create rules for your program that prevent playing on same day as head injuries without medical clearance. If the return to play decision is left to the injured player or team leadership, situational factors such as the importance of the game will impact decision making and put the injured player at risk. By requiring every player who suffers a head injury to sit out the rest of the day, this decision is eliminated and the risk for further injury is reduced.
If you are currently recovering from a concussion, advocate for yourself! Remember, good concussion management should typically follow the formula of a 24-48 hour rest period, followed by a symptom-free, gradual, return-to-play program.
This progression for easing back into sport is included as a quick guide below.

If you seek medical treatment and are not guided through a return-to-play program, you should consider finding a healthcare provider who specializes in concussion. Search for physicians, physical therapists, chiropractors or other medical professionals in your area who specialize in the areas of concussion, neurology, or vestibular disorders.
Disclaimer: The goal of this post is to provide ultimate players with information to allow them to make informed decisions regarding concussions. It is not intended to provide individual medical advice. Seek medical attention if you or someone you know may be suffering from a concussion.
Sources for this post are listed below.
-
Mccrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion in sport — the 5 th international conference on concussion in sport held in Berlin, October 2016. 2020;(October 2016):838-847. doi:10.1136/bjsports-2017-097699
-
Reynolds KH, Halsmer SE. Injuries from Ultimate Frisbee. 2006;105(6):46-50.
-
Yen LE, Gregory A, Kuhn JE, Markle R. The Ultimate Frisbee Injury Study: The 2007 Ultimate Players Association College Championships. 2010;20(4):300-305.
-
Swedler DI, Nuwer JM, Nazarov A, Huo SC, Malevanchik L. Incidence and descriptive epidemiology of injuries to college ultimate players. J Athl Train. 2015;50(4):419-425. doi:10.4085/1062-6050-49.3.73
-
Lazar DJ, Lichtenstein JD, Tybor DJ. Concussion Prevalence in Competitive Ultimate Frisbee Players. 2015:1-13. doi:10.1177/2325967118759051
-
Beidler E, Bretzin AC, Hanock C, Covassin T. Sport-Related Concussion: Knowledge and Reporting Behaviors Among Collegiate Club-Sport Athletes. 2018;53(9):866-872. doi:10.4085/1062-6050-266-17
-
McDonald T, Burghart MA, Nazir N. Underreporting of Concussions and Concussion-Like Symptoms in Female High School Athletes. J Trauma Nurs. 2016;23(5):241-246. doi:10.1097/JTN.0000000000000227
-
Meier TB, Brummel BJ, Singh R, Nerio CJ, Polanski DW, Bellgowan PSF. The underreporting of self-reported symptoms following sports-related concussion. J Sci Med Sport. 2014;18(5):507-511. doi:10.1016/j.jsams.2014.07.008
-
McPherson AL, Nagai T, Webster KE, Hewett TE. Musculoskeletal Injury Risk After Sport-Related Concussion: A Systematic Review and Meta-analysis. Am J Sports Med. 2018:1-8. doi:10.1177/0363546518785901
-
Lynall RC, Mauntel TC, Pohlig RT, et al. Lower Extremity Musculoskeletal Injury Risk After Concussion Recovery in High School Athletes. J Athl Train. 2017;52(11):1028-1034. doi:10.4085/1062-6050-52.11.22
-
Bauer RM, Asken BM, Snyder AR, McCrea MA, Clugston JR, Houck ZM. “Playing Through It”: Delayed Reporting and Removal From Athletic Activity After Concussion Predicts Prolonged Recovery. J Athl Train. 2016;51(4):329-335. doi:10.4085/1062-6050-51.5.02
-
Elbin RJ, Sufrinko A, Schatz P., et al. Removal From Play After Concussion and Recovery Time. Pediatrics. 2016;138(3):e20160910-e20160910. doi:10.1542/peds.2016-0910
-
McLendon LA, Kralik SF, Grayson PA, Golomb MR. The Controversial Second Impact Syndrome: A Review of the Literature. Pediatr Neurol. 2016;62:9-17. doi:10.1016/j.pediatrneurol.2016.03.009
-
Stovitz SD, Weseman JD, Hooks MC, Schmidt RJ, Koffel JB, Patricios JS. What definition is used to describe second impact syndrome in sports? A systematic and critical review. Curr Sports Med Rep. 2017;16(1):50-55. doi:10.1249/JSR.0000000000000326
-
Broshek DK, De Marco AP, Freeman JR. A review of post-concussion syndrome and psychological factors associated with concussion. Brain Inj. 2015;29(2):228-237. doi:10.3109/02699052.2014.974674
-
Dwyer B, Katz DI. Postconcussion syndrome. Handb Clin Neurol. 2018;158(October):163-178. doi:10.1016/B978-0-444-63954-7.00017-3
-
Bloom J, Blount J. UpToDate. Uptodate.com. https://www.uptodate.com/contents/sideline-evaluation-of-concussion#H3194477714. Published 2018. Accessed March 23, 2019.
-
Harmon KG, Clugston JR, Dec K, et al. American Medical Society for Sports Medicine position statement on concussion in sport. 2019:213-225. doi:10.1136/bjsports-2018-100338
-
Buckley TA, Munkasy BA, Clouse BP. Acute Cognitive and Physical Rest May Not Improve Concussion Recovery Time. J Head Trauma Rehabil. 2016;31(4):233-41.
-
Sullivan KA, Hills AP, Iverson GL. Graded Combined Aerobic Resistance Exercise (CARE) to Prevent or Treat the Persistent Post-concussion Syndrome. Curr Neurol Neurosci Rep. 2018;18(11). doi:10.1007/s11910-018-0884-9
-
Thomas DG, Apps JN, Hoffmann RG, McCrea M, Hammeke T. Benefits of Strict Rest After Acute Concussion: A Randomized Controlled Trial. Pediatrics. 2015;135(2):213-223. doi:10.1542/peds.2014-0966
